Office Number: 972.608.1868 | Fax Number: 972.943.8644
×
Home
About Us
Meet Our Doctors
Services
New Patients
View Accepted Insurance
View Forms
Contact Us
MENU
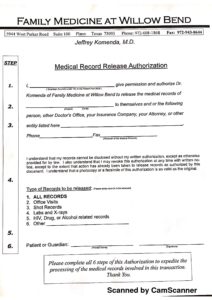
Medical Record Release Authorization Form
©2006-2023 Family Medicine at Willow Bend. All Rights Reserved | Designed By:
Thoroughfare Design Studio
Accepted Insurance:
AETNA
AMERIBEN
AMERIGROUP
ASSURANT
AVAILITY
BLUE CROSS BLUE SHIELD
CIGNA
GREAT WEST
HUMANA
TRICARE
MOLINA
MULTIPLAN
PARKLAND
SUPERIOR
TMHP
UMR
UNITED HEALTHCARE
UNITED HEALTHCARE OPTION
UNITED HEALTHCARE INTEGRATED SERVICES
X